Urinary tract stones are amongst the most painful afflictions of mankind and constitute a major proportion of the workload of an average urologist. For centuries the only relief known was "cutting for stone", an art perfected by the medieval lithotomists, who were for sure, the first specialist urologists. Until the last quarter the last century, open surgery remained the only option in treating such stones. Dramatic changes in stone management have taken place in last two decades, and these days patients with kidney stones usually leave the hospital without a scratch on their bodies !! We will discuss in this article the new concepts in kidney stone management.
How is the urinary system organised?
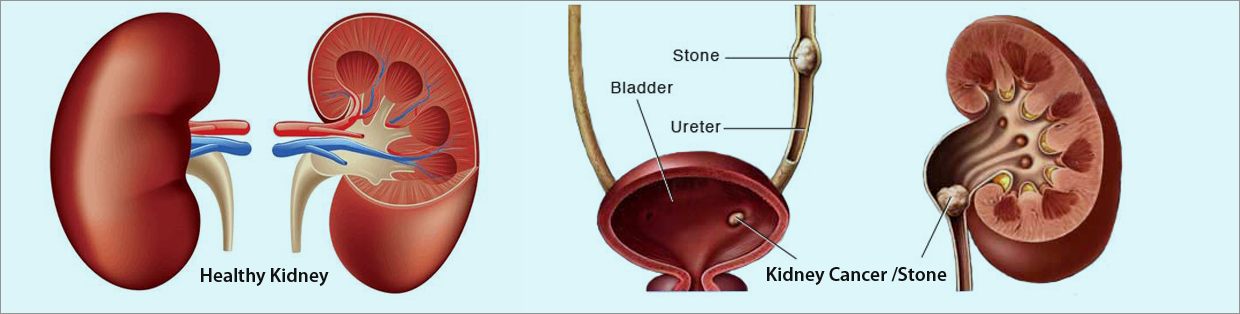
The kidneys are two bean shaped organs situated in the back on either side, behind all the abdominal organs. The kidneys have a rich supply of blood from the heart, and this blood is "filtered" through a system of tiny tubes within the kidney called the "nephrons" or "renal tubules". The waste matter filtered out of the blood is drained out as urine. In each kidney the urine draining out from the tubules is collected into a branching system of larger tubes called the minor and major calyces.
The major calyces join together to form the renal pelvis and from the renal pelvis the urine is carried down by a small tube called the ureter down into the bladder. From the bladder the urine is drained out by the urethra.
Why do stones form?
The cause of urinary stone formation remains the subject of major research. To put it briefly the urine is made up of a number of compounds (solutes) in solution and there is always a tendency for these solutes to crystallize out forming stones. Various agents act as promoters and inhibitors of crystallization. Stone formation is influenced by dietary factors, nature and amount of fluid intake, age, sex, climate, geography, hygiene, race, occupation.
Where do stones form?
Virtually all stones are formed in the kidneys, initially as small particles. These particles grow within the kidney to varying sizes, often filling up the whole kidney as a branched stone (the staghorn calculus). Sometimes they move out of the kidney when relatively small, and then migrate down the ureter into the bladder. As they migrate down the ureter they may block the ureter causing obstruction to the flow of urine: this results in pain which may be very severe (colic). Some reach the bladder, and lodge there, growing larger and larger. Rarely they block the urethra causing a painful retention of urine.
What are the symptoms of urinary stones?
These days silent urinary stones are often diagnosed incidentally in the course of routine health check ups. These stones are usually small, though rarely even large stones may be symptom-free. Stones cause symptoms depending on their location. Thus stones in the kidney may cause a dull ache, a violent colic, an urinary infection or the passage of blood in the urine.
How are stones diagnosed?
An ultrasound examination picks up most urinary tract stones. However a special X-ray called an IVU is usually considered essential in the treatment of urinary tract stones. The urologist will also request urine tests, blood tests, and occasionally more specialised tests like renography/ CT scan/ retrograde pyelography.
What is an IVU?
Is it a dangerous and painful test? The IVU test refers to an intravenous urogram or pyelogram. In this test an iodine containing dye is injected intravenously, usually into a forearm vein. The kidneys excrete this dye, and if X-rays are now performed the structure and function of the kidneys can be assessed. The whole of the urinary drainage system: the calyces, pelvis and ureters are demonstrated on the X-rays. In patients with stones the exact position of the stone can be assessed, and proper treatment selected.
The test may mean spending a minimum of an hour and sometimes several hours in the X-ray department where repeated X-rays are taken. Otherwise this is quite a simple test.
There is a rare incidence of serious allergy to the injected dye, but the modern agents used these days are very safe. The radiologist will discuss the test with you. Please also inform the radiologist if you have history of allergy or asthma.
For the urologist the IVU provides unparalleled information and is often essential.
Do all urinary stones need treatment?
Some stones less than 5 mm in size pass out spontaneously, and the urologist may advise "expectant" treatment. The patient is encouraged to drink plenty of fluids, and is asked to report for follow-up periodically, and surgical intervention considered only if the stone causes symptoms, or remains stationary at a particular location, or enlarges progressively in size.
Is there a medicine for stones?
There is no known medicine that dissolves stones consistently and predictably. One should drink plenty of fluids, and the doctor will advise you about a specific diet if indicated.
What are the treatments available for stones?
The various options available are: lithotripsy, percutaneous nephrolithotomy, open surgery.
What is lithotripsy?
For many centuries surgery was the only option in treating stones that would not pass spontaneously. About 22 years ago the German aeronautics company Dornier, through ground-breaking research, developed the means for focusing external energy to treat Kidney stones and pulverize them to small fragments that are voided naturally with the urine. This was a major advancement, perhaps one of the most significant medical advancements of the last century.
Over the last 20 years lithotripter applications for renal stone therapy have been perfected, and these days lithotripsy is performed as a day procedure in a painless fashion. For this treatment the patient lies on a special couch. X-ray and/or ultrasound are used to target the stone, and by a computerised system the stone is placed at the focal point of the energy source of the lithotripter. Treatment usually lasts about 45 minutes. After treatment the patient rests for a while and then is allowed to return home. Sometimes a "stent" is placed in the ureter if it is anticipated that the stone fragments may block the ureter after lithotripsy. Repeat sessions of lithotripsy may be required, usually not earlier than 5-7 days.
However, all urologists realize that lithotripsy is, sadly not an answer to many of the stones seen in day to day practice. The reason is that for stones that are more than 3 cms in size, branched stones and various other complicated situations lithotripsy is either not effective or is slow to work with patients needing multiple procedures and hospital visits.
In these patients, surgery still remains a valid option. In an average practice in India, where patients present with advanced and neglected disease, at least 40% of kidney stones fall into this category. These larger stones are removed by a new technique called PCNL or percutaneous nephrolithotomy.
Can kidney stones be treated by "microsurgery"? What is PCNL?
Yes, kidney stones can be treated by what is popularly known as "microsurgery" though the correct medical term would be percutaneous nephrolithotomy (PCNL). In this technique the stone is removed by making a small tunnel into the kidney from the back. A fine needle is used to puncture the renal collecting system with the aid of X-ray and/or ultrasonography, and a guide wire is led into the kidney through the needle. This guide wire is dilated and a nephroscope (kidney telescope) is inserted into the pelvis of the kidney. The stones are visualized, fragmented, and extracted, allowing the kidney to be rendered free of stones at the end of the operation in the vast majority patients. This is of course an operation, needing full general anesthesia, average 90 minutes of operation time, 3 -4 day hospitalization and an occasional need for blood transfusion. Patient returns to light work in 7 days time. Nevertheless the operation is safe, for both the patients and the kidney. This operation has really reduced the need for open surgery (cutting surgery), which is now reserved for exceptional indications.
There seem to be many ways of treatment? What is right for me?
Clearly now there is a choice of treatment options for Kidney stones, both to the patients and to the surgeon. Lithotripsy is reserved for the smaller stones. For stones larger than 3 cms in size PCNL is the preferred modality of treatment. The major advantages of PCNL over lithotripsy would be :
- Single procedure complete stone clearance applicable for most types of kidney stones.
- Suitability for therapy of large stones, branched stones, stones in multiple locations of the Kidney.
- Avoidance of repeated hospital visits and less loss of work time.
- The more cost effective option.
- Minimum morbidity, and early return to normal life and work.
How are stones in the ureter treated?
This depends on the size of the stone, and the location of the stone. Small stones, less than 5 mm, often pass spontaneously and may be treated expectantly. If treatment is considered essential most ureteric stones are treated by ureteroscopy. In this technique a fine instrument called the ureteroscope is passed under anaesthesia to the ureter until the stone is reached. Once reached the stone is fragmented with a energy probe. The most common form of energy probe used is the pneumo-ballistic lithotripter which works on the principal of the pneumatic drill. Other energy sources for lithotripsy within the ureter include ultrasonic, electrohydraulic and laser devices. After pulverisation the stone fragments are washed out or extracted, and a fine tube (stent) is left in the ureter (usually) for a few weeks. Very large ureteric stones may be removed by open operation or by laparoscopy.
Can stones form again after complete removal?
The answer unfortunately is yes, even if the stone has been completely removed. This is because the factors that cause stone formation persist. The doctor will probably investigate you thoroughly for biochemical abnormalities that cause stone formation and then advise you about the any diet changes that you may have to make. A high fluid intake is routinely advised. You will also need to be followed up closely.